Honouring Strength: Overcoming Addiction Identities
Adapted from Thesis, by Jeff Talbot B.Sc., BSW,
MSW Cand., RSW
I bought into this belief that everything I was, was because
of alcohol. So I was basing who I believed I was on my supposed
greatest weakness. Now that’s tough. How do you get ahead?
(Judy)
My thesis explores how some people manage their relationship
with / without alcohol in ways that do not seem to harmonize with
status quo discussions of alcohol abuse and recovery. My question
was: How do the experiences and needs of those overcoming addiction
independently of 12-step / disease-model culture impact social
work practice? This qualitative study explores experiences of
seven "outsider" participants. Two quit drinking completely without
the help of addiction therapy or self-help groups; the remaining
five participants reclaimed a manageable relationship with alcohol
after years of dedication to 12-step programs. The participants’
experiences are explored using a social constructionist cultural
model. Issues regarding the political context of addiction counselling
are explored, and implications including assessment and resource
development for social work practitioners are discussed.
After 20 years as a social worker / alcohol and drug counsellor
in northern British Columbia, my practice has been greatly impacted,
strangely enough, by political rhetoric. After earning a degree
in psychology, I found that strategies I learned were not acceptable
to the support agencies in the town where I started my career,
unless they were within the theoretical boundaries of the disease
model and the 12-step approach to treatment for "alcoholics" (a
self-proclaimed title). I understood the practical reasons for
this policy; essentially, before alcohol and drug counsellors
were available, the local community depended on Alcoholics Anonymous
as the only support for people with alcohol problems. Later, as
I earned my BSW and moved to a somewhat larger northern community,
I found there was more room for a variety of approaches in a multi-staff
alcohol and drug counselling office. I found that, as a result,
I had a front-row seat to the political turf wars between multiple
recovery cultures. Polemic disputes occur on several levels. One
concern is over the ethical dilemma of client self-determination
versus a prescriptive disease model that assumes that "insanity"
and "denial" (terms often used in 12-step literature) preclude
the client’s capacity to make healthy choices. Another level
relates to policies and practice of harm reduction versus zero-tolerance
and tough-love approaches. The conflict also highlights disputes
about the context of expert knowledge (those with personal experience
versus those without). The fundamental issue is the debate over
alcohol addiction as individual experiences of one truth, one
journey, and one solution informed by pathologizing practice,
versus a perspective of addiction as individual experiences with
multiple knowledges, journeys, and many uncharted territories
where outsiders find themselves (Korzybski said that "the map
is not the territory" (Truan, 1993). Consequently, the uncharted
is beyond the conception of the rhetoric commonly used to understand
the experience of addiction).
People have been coping with the negative consequences of
drinking alcohol since the beginning of civilization. However,
how these causes and consequences associated with drinking problems
are defined varies according to culture. For example, modern western
perspectives of alcohol addiction management are heavily influenced
by medical positivist research (Peele, 1989). In contrast to positivist
traditions, cultural studies theorists (Alasuutari, 1992; Bannerman,
2000; Denzin, 1993; Gusfield, 1996; Pinderhughes, 1989) have played
an instrumental role in informing my research of alcohol problems
and recovery. As Pinderhughes (1989) observes, "Culture determines
how we see a problem and how we express it¼
" and culture can "determine what specific symptoms people experience,
whom they seek out for help, and what they regard as helpful"
(p.13). Key concepts that are useful from cultural studies include
the valuing of discipline-jumping and genre-jumping; bricolage;
polyvocality; and incompletion or non-closure of knowledge. These
concepts embrace some postmodern assumptions: that reality is
subjective in relation to our experience, and that experience
is informed by more than one framework. Consequently, knowledge
itself is as relative as our self-awareness in relation to people
we observe (Furman & Ahola, 1992; O’Hanlon, 1993; White,
1993).
This study was developed based on a relatively regular phenomenon,
which has fascinated me throughout my career as an addictions
counsellor. I have witnessed individuals who were able to establish
a more meaningful identity in relationship with alcohol after
many years as an "alcoholic" or "alcohol-dependent" person. This
has occurred in spite of a general belief among addiction treatment
professionals that those with serious substance abuse problems
warrant a "substance-dependent for life" label. Consequently,
these persons achieved their success by methods outside the boundaries
of traditional disease rhetoric and intervention.
The controversy created by outsider experiences reflects,
from a cultural studies perspective, the influences of more dominant
cultures and how these ideas seep into the community in which
this study was conducted. Dominant ideas are sold through a market-driven
deluge of television shows, magazines, music, and newspapers.
This subtle or overt propaganda is disseminated through many modes
and role models. For example, a key character in the award- winning,
long-running ABC network television series NYPD Blue(episode
65, "Closing Time," broadcast on May 14, 1996, written by David
Mills and directed by David Rosenbloom), detective Sipowicz (played
by Dennis Franz), suffers loss of control over his drinking. The
character’s capacities deteriorate until he surrenders his
will, asks for help, and rejoins AA. In this series, Sipowicz
also tries to sponsor another department member. This plot depicts
the classic American disease model view of anyone with a drinking
problem. Many depictions of alcohol or drug problems as viewed
from the disease / recovery culture are demonstrated in popular
culture, from major motion pictures such as Leaving Las Vegas
(Figgis, 1995), Clean and Sober (Howard, 1988), and 28
Days (Thomas, Topping, & Grant, 2000), to television episodes,
to themes and images pervasive in most forms of media. Marketers
for brewers or distillers construct dream sequences of bikini
or Clydesdale teams on the air to remind the consumer that the
good life happens with alcohol. The consumer’s boring lifestyle
is shaken, not stirred. The capitalist prerogative to saturate
markets for profit continues, neither acknowledging nor taking
responsibility for the consequences. Whereas marketing discourse
serves to popularize drinking, alcohol problems are marginalized,
objectified, and relegated to the gaze of medical discourse. To
have a problem with alcohol is to be abnormal. The message is
that if you join a fellowship, abstain, and toe the line, perhaps
you will be redeemed, or at least viewed more acceptably, like
detective Sipowitz. How does this polarized perspective serve
the needs of persons who seek help? What is the role of the social
worker?
The field of addiction treatment has often been described
as a multidisciplinary setting, with competing etiological assumptions
and theoretical applications concerning addiction and therapy.
Since the inception of the Alcoholics Anonymous fellowship in
the 1930s, there has been significant progress in the development
of therapeutic methods to assist individuals with alcohol- or
drug-related dependencies (Baker, 1988; Berg & Reuss, 1998;
Blum & Roman, 1987; Chang & Philips, 1993; Roberts, Ogborne,
Leigh, & Adam, 1999a). Nevertheless, in North American culture
the concepts of the disease model and 12-step program treatment
dominate (Kaiser Foundation, 1997; Lender, 1979; Roberts et al.,
1999b). The culture of the disease model and the 12 steps of Alcoholics
Anonymous tend to predominate and marginalize alternative options
in northern remote communities.
For many who overcome an addiction habit, personal identity
relating to the process of recovery changes over time (Sommer,
1997). Others who face addiction and are adversely affected by
the dominant practices of the "recovery industry" (Peele &
Brodsky, 1991) find alternative ways of healing. Whereas society
often marginalizes the addicted, 12-step discourse often further
marginalizes those who do not conform to the accepted etiological
assumptions and resulting implications of the program (Granfield
& Cloud, 1996; Kearney, 1998a; Peele & Brodsky, 1991).
In spite of pressure toward conformity in the culture of recovery,
there are those who have success in overcoming addiction in their
own lives outside of a 12-step program or formal treatment (Anderson,
1994; Granfield & Cloud, 1996; Kearney, 1998a).
These stories of outsiders who eschewed the alcoholic-in-recovery
identity may reflect a self-perception based on strength and capacity,
turning away from a deficit identity. Some of these people tell
stories about learning to accept love, and about taking responsibility
not only for their potential worst, but for their best as well.
These persons seem to have developed a maturity and insight that
comes from years of personal work and growth. One participant
described a journey of discovery for the love within himself he
knew wasn’t afforded him as a child. Others describe their
families as their greatest strength, and that placing the family
first affirmed all of the love, support, and incentive needed.
Still others found that stepping out of the culture of recovery
was necessary to reclaim their creativity and find love. Other
qualities included demonstrations of strength, commitment, compassion
and consideration for others, and a potent determination to never
again give up their right to decide how to view the problem, or
the solution. Outsider recommendations invite reflection on what
it means to offer a no-harm practice; I believe we do no harm
whatsoever to our clients by identifying, amplifying, and celebrating
their strengths and capacities.
The information described from the experiences of these people
may have some interesting implications for social work practice.
These insights may also have meaning outside of the boundary of
discourse on alcohol problems and recovery, in that some of the
participants’ stories reflect a similar context of struggle
experienced by others, such as people with drug problems or smoking
and eating disorders.
Method
The research question I developed for this study was, how
do the experiences and needs of those overcoming addiction without
the 12-step / disease model culture impact social work practice?
I conducted an interview study with seven participants, using
a flexibly structured interview process in order to ensure participant
experiences would be documented in their richest detail, in relation
to the objectives of this research. The social constructionist
(where meaning is negotiated in discourse) design was intended
to invite participants into a "co-authorship" relationship, sharing
power and insights. This "co-authorship" function was supported
through a member-checking follow-up discussing and negotiating
the results of a retrospective analysis of problem severity and
a thematic analysis. The "co-authorship" intention of this research
is demonstrated through the use of participant quotation as much
as possible to ensure that experiences, theoretical developments,
arguments, and other insights could be credited to each of the
participants. The use of quotation would also serve to distinguish
my voice in the research from theirs - enhancing reflexivity,
as well as the credibility and transferability of the participants’
experiences.
Due to the politically controversial nature of this research,
I chose to conduct a retrospective analysis of problem severity,
in order to address the argument that participants did not suffer
from serious alcohol problems. I documented, through personal
review of interview transcripts, the extent of alcohol-related
problems apparent in each participant’s narrative. I developed
the units of measure for this analysis by adapting criteria from
the DSM-IV-TR, which is widely accepted in addiction assessment
discourse. I did not use the specific substance dependence criteria
from the DSM-IV-TR, to dispel any assumption that the participants
in this study could be diagnosed as substance dependent. This
analysis was limited to the presence of evidence within each participant’s
narrative that satisfied each of the adapted criteria.
I also conducted a thematic analysis; however it was
not my intention to attempt an exhaustive, complete description
of participant narratives. According to the social constructionist
view that meaning is a dynamic, ongoing negotiation within discourse,
the notion of completion is an unobtainable goal. I ended the
analysis development when the information from each participant
had been thoroughly reviewed according to the objectives I developed
reflecting the research question. Furthermore, I chose not to
overly interpret participant experiences through the thematic
analysis, preferring instead to use quotation from the participants
to allow their direct input to discourse with the reader. I believe
that this decision supports the integrity of the social constructionist
process, the wisdom of the participants, and the imagination and
critical judgement of the audience.
There were, in the end, seven participants. In retrospect,
I believe I could have found many more outsider interviewees
who would have shared their divergent success stories. Five interviews
were conducted face-to-face, one by telephone, and one via email.
Interviews (other than the email process) were audiotaped with
participant permission, and transcribed.
I managed to contact six of the seven participants for the
purpose of member-checking, after providing each of them a copy
of their transcribed interview and a draft of the thematic framework
I had developed. Each indicated they believed the model I used
accurately reflected her or his personal experience and perspectives.
One participant did not respond to my package nor to several phone
messages. Since this person had been provided several means to
contact me, had been briefed prior to signing the consent to participate,
and had been informed of my timeline, I assumed that her silence
did not constitute her withdrawal as a participant. She received
a copy of the finished thesis as mutually agreed.
The participants in this study have all experienced serious
alcohol problems, ranging from tolerance and avoiding important
events because of drinking, to withdrawal seizures. However, the
retrospective analysis was controversial for the participants.
Beth, (all participants have been given pseudonyms), provided
some feedback regarding this analysis which I believed reflected
a common concern participants had, over a process which involved
potentially pathologizing practices:
The criteria, like other mental health assessment tools, need
to take into account cultural, identity, and spiritual (including
personal values) aspects of the person being tested. I once had
a friend in class practice a new mental health assessment tool
on me. I asked her before I filled it out, "Do you want me to
answer like a client—like how I think it should be done,
or do you want me to answer honestly (including spiritual experiences)?"
She smiled and told me to answer honestly. So I did. My diagnosis?
Schizoid and dependent. Was she ever shocked! How could her test
say this? She had no clue as she thought that I was pretty functional.
I smiled back and told her that her test is designed for one culture
group and that she told me to be completely honest. The results
would have been different if I was answering like I thought I
should be (according to the culture behind the test design). How
true is that? Do I really need to be walking around with those
labels?
I think it is important to understand that I am
not a certified diagnostician, nor did I approach this analysis
from a completely neutral and objective position. Moreover, there
are obvious weaknesses in retrospective self-reports, particularly
concerning descriptions of character blemishes, and especially
regarding recollection of events over a decade old. It was my
intention that this exercise would provide evidence to caution
any assumptions trivializing the impact of participant histories
with alcohol.
I attempted to create a framework to describe participant
experiences, and came up with a map (Figure 1) of the model I
developed for the purpose of organizing information from participants’
narratives:
Figure 1: A Model of Social Construction, Identity
and Culture
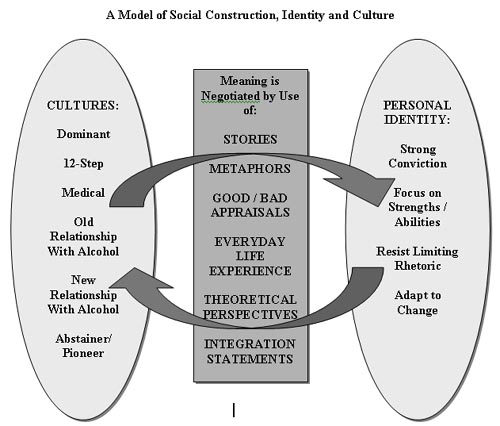
The model I developed is somewhat simplistic; I began with
the social construction concept, mapping the process of negotiating
meaning through discourse. Within the social construction process,
each interview had moments when the participant was her or his
own narrator. Consequently, each story was grounded by descriptions
of self, the "I," a dynamic focal point that I referred to as
personal identity. The participants’ conversations reflect
their present sense of identity, situated in the present, in context
to their story and their visions for the future. Their narratives
include stories of their experience with different alcohol-related
environments, which I have argued can be considered as cultures.
Different rhetorical frameworks such as the disease model and
the philosophy of the Alcoholics Anonymous fellowship also inform
discourse according to each view of people attempting to overcome
alcohol problems. I chose to describe these different perspectives
as cultures as well. For example, all participants spoke about
living in modern society, which I refer to as the dominant culture
(Fillingham, 1993; Rabinow, 1984), and about their "old relationship
with alcohol," which involved other people, rituals, practices,
and meaningful experiences. Whereas some participants speak of
a new life without alcohol (which I termed "Abstainer Pioneers"),
others speak about entering the fellowship of Alcoholics Anonymous
or other 12-step programs and later reclaiming their ability to
drink responsibly (which I termed "New Relationship With Alcohol").
Each of these situations involves other people, specific rituals,
practices, and meaningful experiences. Viewing these different
milieus as cultures has been accepted practice (Alasuutari, 1996).
Participant narratives provided information that suggested
some similar experiences. I have categorized experiences relating
to personal development and self-concept, such as "strong conviction",
"focus on strengths / abilities", "resist limiting rhetoric" and
"adapt to change". Other experiences that related to environment
and lifestyle I depicted as other cultures. Consequently, personal
experiences outside of the aforementioned cultures, such as the
12-step fellowship, could be recognized as contributing factors
in the mediation of identity.
Although the participants’ narratives resemble a generally
linear storyline, each person’s current identity has been
cumulatively impacted by their experience within each of these
cultures. Each of these cultures’ perspectives relating
to a person’s current relationship with alcohol, whether
abstinence or responsible use, is a mediating factor in the person’s
self-concept and their identity as they adapted to a new lifestyle.
Consequently, there is an ongoing relationship between personal
self-concept and different cultures, proportional to the person’s
experience, where meaning and consequent identity integration
are constantly negotiated.
For the purpose of this model and the analysis, I considered
the tools used in the mediation and expression of culture and
concepts of personal identity. Common methods I noted included
story, metaphor, good or bad appraisals, description of everyday
life, theoretical view and development, and the integrating statements.
Stories
Each participant’s narrative is a story in itself,
and within each narrative are many stories that help to situate
the person in his or her context, relating to the surrounding
culture that he or she was immersed in. These stories are the
allegories that inform the listener about the significance and
the meaning attached by the teller. They are the building blocks
of these people’s messages—their most vital tool in
communicating their experience. Consequently, participant stories
have been constructed in a manner specific to this research, and
would have been constructed differently in another situation.
Metaphors Reflecting Culture
The use of metaphor, a figure of speech where one word
or phrase is used to imaginatively but not literally replace another,
has been a significant and long-standing tool of qualitative research
(Gubrium & Holstein, 1999). In recovery culture, one can expect
to find a rich and seemingly endless number of metaphors (or codes
and ways of decoding cultural insiders’ constellations of
meanings). Each one is essentially a story unto itself; perhaps
it is an allegory with a moral or an in-your-face political message.
These metaphors are the shorthand of the political rhetoric of
recovery, which involves major transformations, such as the emergence
of a new identity, or profound shifts in the perceptions and practices
of everyday life. These metaphors can describe experience across
cultures, such as Joe’s:
Like my AA buddy, who is hard-ass, hard-core AA, has no
concept of his motives, although he’s learning. I can’t
help but love the guy. But we have another connection. We met
in school, when I was making a career change. We have a bond that
is from being in another trench. From being in the school trench¼
(Joe)
Or the recovery metaphors can be cloistered within a
culture, closed and cryptic, such as "A friend of Bill’s
(in reference to Bill Wilson, one of the founders of Alcoholics
Anonymous,)", "I took the pledge," "disease," "cunning, baffling,
and powerful¼ " "the word of recovery."
Such metaphors mark insiders to each other, and exclude those
who are outside of the culture of AA. Other metaphors can also
provide a powerful indicator about how the teller views his relationship
with the problem, the culture, or another relationship, such as,
"I was firmly captured and imprisoned by the alcohol"(John).
Good / Bad Appraisals
Appraisals are a significant part of the process of
moving from one culture to the next. They can provide a method
of preparation for migration similar to Smith and Winslade’s
work (1997), grounded in a number of practical models assessing
change, such as motivational enhancement (Miller & Rollnick,
1991) and the transtheoretical model (Prochaska et al., 1994).
Participant stories tend to indicate the level of commitment a
person has in a culture by the preponderance of positive appraisals
about the culture, relating to her or his identity. Judy spoke
about AA, and stated:
Theres no doubt it helped me, theres no doubt about
that. It gave me people to be with that were trying to stay sober
too, which is what I needed and they supported me. And I think
thats AAs absolute biggest asset: people caring. And it put
me on some paths that I wouldnt have explored if I hadnt been
there, like spirituality. (Judy)
Stories reflecting outsiders’ ambivalence tend
to include more of a balance of good and bad appraisals for different
cultures. John gave a poignant example during a moment of reflection:
It makes me think back to that old story about AA, "once
an alcoholic, always an alcoholic," right? And I dismissed that,
at one point. But I need to know under new evidence, re-evaluate¼
Because I certainly dont want to be going back to where I came
from. But saying that, that little voice of alcohol pops up and
says "maybe." (John)
Exit stories tend to reflect a shift of appraisals, with
the bad ones describing the culture being left behind, and the
more positive stories describing the culture they are moving to.
These positive appraisals often incorporate powerful reflections
of personal strengths and identity. Joe provides another excellent
example:
I stepped off into the world. I couldn’t stand the
hypocrisy. And you know what? At some point someone came along
and said to me, "Well, you know, these [meetings] are great, but
you get healthy here, and then you move on." And it was a seed
that they planted in my head. It was just a thought, just an idea.
It sat there, and suddenly I realized that I can’t stay
here forever. (Joe)
Participants who have settled into a new, possibly outsider
identity over time may begin to use positive appraisals about
former cultures, in proportion to the number of ideas from the
culture they have been able to incorporate into their new identity.
These appraisals are indicators reflecting the negotiation of
meaning between cultures and personal identity. Judy reflected:
And you know, to give AA their due I learned some good
things there, too. Like ways to deal with fear, and just all the
things life brings at you¼ the "one
day at a time," that’s good advice for anyone. (Judy)
Everyday Life Experience
Everyday life experience is the common ground between
personal experience, social and cultural context, and theoretical
perspectives (Alasuutari, 1992). John provided a poignant picture
of living in a world of hopelessness:
I tried suicide¼ because to
me at the end I termed it being between the proverbial rock and
a hard place. I took the gun out, I loaded it, I stuck it in my
mouth¼ and I couldnt pull the Goddamn
trigger. I was scared of living and I was scared of dying and
I had nowhere to go¼ For me, even when
I wasnt drinking, I could be out on a beautiful sunny day like
this walking down the road and it would actually look grey. It
was just dull. And that was my whole affect, right? I know, my
first sponsor, he said he used to watch me walk by and I never
looked up. I was watching my feet, walking down the road¼
(John)
These are the parts of a person’s narrative that provide
the witness with a window to life at that time, and provide an
illustration of how different cultures and political views look
and feel as normal, everyday experience.
Theoretical Perspectives / Developments
As a person migrates from one culture to another, explanations
become a natural part of integrating the process. It is noteworthy
to consider the migrating person’s explanations from the
perspective of the different cultures she or he is negotiating.
These explanations are the core of the social construction process.
This is where political rhetoric crashes into personal reality
and anecdotal truth. For example, George described his personal
model of addiction as, "I believe it’s a mental thing,
not a physical thing, in that sense. I figure that if it’s
mental then you have control over that, as a person." Georges
theory is his practical explanation of his success in abstaining
without help. If the reader reflects on his perspective in contrast
with the deficit-identity messages of the AA fellowship, the implications
of rhetoric on the persons identity and attributions of success
become more apparent. Other statements that exemplify participants
outsider theoretical views include "The pain and anxiety of
growing up in that household, that’s why I drank," (Joe);
"Alcohol, it isn’t the substance that’s the problem,
it’s the user" (Joe); "It’s about a number of things.
It’s about running, it’s about not facing reality.
It’s about fear. It’s about pain" (Claire).
Integration Statements
Integration statements are affirmations regarding self-concept
in relation to cultural influence. These are the statements that
reflect upon what a person’s story is telling her or him
about who she or he is as a person. Many stories end with integration
statements, whether these stories are allegorical or about the
living journey itself. Integration statements are often reflective
potent descriptions, with a focus on what is and leaving behind
what isn’t. These statements can also reflect fundamental
understandings about need, hope, and acceptance, and can be spiritual
affirmations: "Let’s say I was an alcoholic" (George);
"I’m one of the strongest people I know" (Joe); "The choice
I made I feel great with," and "I didn’t make this
decision thinking everybody was going to accept it. I didn’t
make it for them, I made it for me" (Claire).
I have identified and described these different processes
of negotiating and expressing meaning as if they were mutually
exclusive; obviously this is not the case. These processes are
more than the sum of their parts, and they are interconnected;
it would be unlikely to have integrating statements without inferring
some theoretical view, good or bad appraisals locating self-concept
in relation to political rhetoric, or without the use of metaphor.
Wrapping the entire context of a person’s identity and journey
into the label "story" seems to trivialize the person’s
experience and meaning. A story is just one description of the
complexity of one’s experience. It is the profound nature
of the experience that makes these stories so rich and provocative.
Culture
Each participant story of experience reflects more than
one culture, and some reflect the influences of more cultures
than are within the scope of this study, including cultures of
ancestry, career (for example, families of railroaders), or gender.
The process of describing the different cultures in the participant
stories resembles a general map of the journeys the participants
took, implying an archetypal story worthy of Ulysses’
narration. However, "the map is not the territory." Although the
description of the different cultures is offered sequentially
as a general narrative roughly similar to these participants’
experiences, this framework should not be considered as a grand
story but rather as a reflection of each participant’s identity
development in relation to the impact of different cultures over
time. Each participant took her or his own journey toward a better
identity.
Participant Recommendations to the Helping Profession
Participants offered their own ideas about what they
felt professional practitioners need to know in order to help
others struggling with addiction problems. Here’s what they
had to say.
Joe’s response addressed his own experiences with counsellors:
If you choose to be in social work, or a counsellor or
something, you’re choosing to help people. Then you better
have helped yourself.
¼ And so as a professional¼
when you are the resource broker, and you are trying to allocate
resources, how do you fit a person like me into that system? I
don’t know. Advice? I still honestly have to say, I think
[pause] you need to have done some of your work. No perfection.
And suspend the judgement. I think that if you have done your
own work I think that you can easily suspend your judgement.
¼ Thats been my absolute best
experience, a group situation. It was a project. It had a beginning,
a middle, and an end. Okay? And then you move forward. And the
worst part about AA is that, here I amI want to quit drinking
and then theres the rhetoric that these people are trying to
pump into me, that, "Oh, youre here for life." Why the hell do
I wanna be around a bunch of hypocritical people for the rest
of my life, with the threat that if I have another drink Im going
to die? I mean, how coercive is that? A beginning, a middle, and
an end. And then you have to step out and try what youve learned.
(Joe)
Joe implied the need for professional helpers to understand
his theoretical framework: that addiction is merely a destructive
solution for underlying issues. While Judy provided some hints
at her own etiological assumptions about addiction, her advice
is simple:
Ive got a bit of a biologist, science kind of slant with
my work, and I dont believe its a disease until I have the proof.
You know what I mean? I think that definitely there is a
chemistry difference between people with addictions and others.
But that’s all addictions, be it whatever. And I think that
hopefully, eventually medical science will be able to address
that. And not by Band-Aids; you know, giving people mood-altering
drugs and so on, but by giving people naturopathic diets that
give them whatever’s missing that causes that imbalance.
That’s what I’d like to see; that would be my answer
to your magic wand question.
You asked a question about what could help doctors and psychologists
and social workers and people like yourself to do better? The
only thing I have to say, is give people the room to do whatever
works. (Judy)
Judy’s last statement implies the need for
client-centred practice; giving people the room to do whatever
works requires providing therapeutic space to respect the client’s
perceptions of problems, solutions, goals, and outcomes.
George’s response to the question, "What do you think
that professional people (social workers, therapists, and the
like) need to know from your experience about overcoming addiction?"
was powerful:
I think [pause] as witnessing the Ministry’s [of
Children and Family Development] problems that they have—they’re
understaffed, they’re underpaid, and they have one social
worker for two handfuls of kids. They cannot protect them all,
they cannot be eyewitnesses to everything that goes on in the
houses were they are.
They need somebody [pause] to go around to these places and
[pause] take every little issue that these kids have and take
it seriously. [pause] Don’t take it with a grain of salt.
Don’t take it that you’ve heard it [pause] from other
kids or whatever. Listen to the kid, ’cause the kid is trying
to tell you something. And if it is alcohol-related there is a
reason why, there is a reason this kid is drinking at 12, there
is a reason this kid is doing drugs, there is a reason she is
on the street selling her body.
And it’s not even in the foster homes; it’s in
every home. Like I know friends of [name] that are, you know?
You just want to scream, at some of the shit that goes on with
their parents, you know? And what can you do about it? I know
society has come along way from [pause] listening to your neighbours
fight and get into a fistfight and the husband is yelling at the
wife and all’s you do is close the window. But it still
goes on, you know?
I just [pause] I just wish that the kids that are in trouble
would get help earlier. A lot of them. Because nine times out
of ten, when they do get help it’s too late.
I wish that [pause] that somebody would have taken an interest
in me as a young child and done that sort of stuff with me. I
mean, somebody I could look up to and say he does drink and party
and he’s got a good home life and [pause] he’s got
a job [pause] and you know [pause] something that I could look
forward to that way. Where all I had were my friends, and alcohol
was their buddy as well as mine¼
Yup that was the gist of it. I feel that [pause]
that kids today, they’re probably in worse than I ever was
because before when I was going to school, you know everybody
partied on the weekends and stuff, but drugs wasn’t the
problem that it is today. Kids, you know [pause] you got to get
to them early in my eyes. (George)
George’s response reflects his values about nurturing
children, which he believes needs to be the principal focus for
preventing or reducing the harm of substance abuse.
Gina’s answer, in response to why she decided to participate
in this research, reflected a holistic worldview, addressing everything
from the desire to live to self-care:
Youre going to pass it along, and maybe somebody will
benefit from it, theyll be open about themselves, and, just spewing
your guts out about what your problem is. Dont be afraid, dont
try and hide it. You want to do something. Everyone wants to help
themselves, nobody wants to die. Nobody wants to.
Wherever there’s life there’s hope, and I’ll
always remember that. And that’s what these people should
be saying. "Let’s see about what we should do." Just remember
that they don’t want to die. You know, there’s hope.
Physical health is very important, three meals a day, especially
for someone that is drinking, that doesn’t want to quit,
they should have three meals a day, and take vitamins. And when
you do decide to quit drinking, you have a better chance of survival,
physically when you do go into detox. It’s very important
to have your daily nourishment. And the more you eat the less
you drink. And then even if you do drink just as much, the food
helps to absorb the alcohol.
I think if your body’s well nourished, you’ll
go out and do things; be more active. And when you’re not
eating properly you’re sitting there with a can of beer
or something, and neglecting the kids. If you’d have kept
your health up you could be doing things with the children. Well,
my children are my pride! (Gina)
Ginas response reflects the need to recognize and develop
goals with people in a holistic manner, addressing issues from
physical health to a healthy environment, parenting, and hope
that provides motivational and spiritual grounding for a person
to reclaim a life worth living.
John’s insights underscore the need for patience, persistence,
and empowering people who are overcoming alcohol problems:
I think the most important thing I think for people working
with people with alcohol and drug problems is it’s a process.
Relapse is normal. I’m trying to think if I know of even
one person who never had a relapse. Including myself up till the
time I actually got it, like I tried to quit a hundred times.
You know? It didn’t work. ’Course I wasn’t trying
to get any support or figure out a way to do it, I was just going
to stop drinking.
Well that didn’t work. So I think it’s important
to understand that it’s a process and it takes time and
it’s the whole piece of the person has to be with it. It
has to be integrated with their physical well-being, their spiritual
life, or getting some sort of spiritual connection; [pause] not
necessarily in the AA sense, but just in the sense of becoming
comfortable with self.
Because if you’re not comfortable with yourself you’re
going to take something to change how you feel. I think there’s
a lot of core stuff around that and people need to be supported
through it and it can be a very frustrating experience for people
trying to work with them who want quick change cause it doesn’t
happen that way. It just does not happen. So patience and caring.
Caring for them all the way through it and if you do that long
enough you’re going to see some of them change.
And give them power. Give them their power. And that’s
one of the things that AA takes away, it dis-empowers. Turn your
power over to this higher power which means you’re weak
and powerless so, and I think people need to get control of their
lives and I think that’s part of what happens after five
or six years; they take their power. They get on with their lives.
That doesn’t mean that you can’t have a spiritual
connection or whatever it is but it also means that you’re
aware of your own, where you do have some power. (John)
John’s advice reflects Gina’s ideas about
working from a holistic framework, and Joe’s theoretical
view that addiction masks underlying issues. I infer that his
thoughts about patience and perseverance, about the non-linear
process of recovery, and the need for empowerment suggest client-centred
approaches. "Give them power" implies the concept of therapy as
a political act, a perspective amenable to feminist and narrative
therapeutic frameworks.
Claire, responding to the question, "Imagine that you have
been given a magic wand, which will help you create the ideal
circumstances for people like yourself to resolve their addiction
problems. What would you like to do?" demonstrated her insight
as a practitioner:
What would I do? Oh wow, that would be so much fun! I
would have everything in one centre. And what I mean by that is
after they were all detoxed and stabilized and all that kind of
stuff, instead of just preaching the 12-step programs, going through
the little alcohol and drug system during recovering planning,
I would have them meet people in the programs that were¼
. Say the 16-step empowerment program because it’s a lot
different than a 12-step program. And yet they would meet the
12-step program people. They would meet people who are doing what
I’m doing today. Like harm reduction I guess would be the
word cause I can’t really find a word for it. Yeah, so they
would have all the choices, all the time in the world right? You
can learn about them all, and they all have their own little workers
of course, [laughter] cause we got lots of money. One-to-one here,
who had no opinions except to totally inform them and completely
empower them to make their own choices. Then I think people would
get recovery, but it costs a lot of money. Because I think that
when we’re making choices for other people we’re not
empowering them so we see them over and over and over again. But
I also think they don’t have the money to do that, right?
Well, no magic wand? The next best thing would be what I
try to do. Is still informing people. Information taking, understanding
people for where they’re at I think is the key. I believe
that referral is very important. I mean, I do recovery plans with
20 people a day. And they listen to me and most of them just do
whatever because they don’t know. So if I’m being
the best I can be that day, because I’m not overworked,
without the magic wand I guess, just time and really informing
them. Instead of saying, "Well this is our system of care, you
should go from here to this 28-day program, support recovery program,
then this 30-day treatment program, and ¼
" Because that’s what’s there.
Everybody is an individual. Yeah. If my experience could
stop those people [professional practitioners] from clumping people
with addiction issues into one certain criteria. I mean, especially
if you’ve been in the field for a while it’s hard
as human beings not to expect people to be a certain way. So that
would be for right across the board for them to absolutely listen.
And understand a person’s individuality, because if that
happened, then I guess decisions based off that would be thoroughly
off the person’s needs and only the person’s needs.
And not what has been normal or accessible or affordable. (Claire)
Claires professional advice to colleagues strongly promotes
client-centred practice: to eschew assumptions that clump clients
into one category, to understand a persons individuality, to
absolutely listen, completely inform, and completely empower.
Claire recognizes the authority of her professional status, but
argues that decisions need to be made based only on the persons
needs, which I believe would take priority over the dominant discourse
of institutional privilege. Claires belief in referral implies
a professional duty to help situate clients back in their lives
with resources that fit their needs.
Beth clearly provides an invitation for practitioners to
accept and support clients who need to find their own path to
a better life:
The ideal circumstances for people like me to resolve
addiction problems would be to work with someone and /or a group
that is not going to try and peg me into an already set pattern
of use and that has the attitude of exploring who I am, what I
need, what and how to be happy, healthy and fulfilled in ways
that are not going to hurt me or others. A program of some sort
that teaches ways of living in the world. This scenario would
be expanding, empowering, and full of experiments. It would be
far removed from disease and a continual alcoholic identity.
Professional people need to know how to respect and honour
my experience in overcoming addiction. This means cultivating
an attitude of being present, curious, and knowing how to listen.
They need to be quiet, focused, and aware of their own feelings,
programming, and experiences. The helper’s reference point
may not be true for the individual who is sharing.
As a final point, I believe healing from an addiction involves
accurate knowledge, the permission to change strategies, refresh
old ideas, and most importantly people who are genuine and who
can listen without judgement. (Beth)
Beths advice also promotes self-determination reflecting
client-centred practice, but with a distinctly postmodern flavour.
She suggests a focus involving a counsellors intimate self-awareness,
genuineness, and listening without judgement; and a process that
eschews deficit rhetoric and promotes experimentation and exploration
of needs, identity, and fulfillment in the context of the world.
When I reflect on these persons’ narratives and their
suggestions intended for the professional practitioner reading
this work, I believe they are asking to be listened to and respected
as individuals, and to not be judged. I believe they meant that
they’d like their issues to be treated in a manner that
respects their individuality, and not as problems that fundamentally
limit how they should see themselves. I believe they respect practical
solutions for alcohol problems, including abstinence, especially
in the beginning of the process of reclaiming their lives.
Theoretical Implications of this Research
Participant experiences challenge a number of "one size
fits all" theoretical tenets grounded in the etiology of alcoholism
as a disease. Specifically, in spite of personal histories of
serious alcohol problems prompting professional assessment and
referral to AA, some participants’ current relationship
with alcohol is not characterized by compulsive use, loss
of control, nor progression. Four out of the five participants
who chose to experiment with controlled drinking have managed
to do so successfully for a period of time ranging from two years
to more than a decade. These four participants indicated that
they control their alcohol consumption and have not experienced
compulsive urges or negative consequences attributed to their
drinking. Consequently, there is no evidence of the phenomenon
of progression. The fifth participant, John, who was ambivalent
about his alcohol use, has made some significant changes, is now
abstaining (without using disease / 12 step rhetoric), and enjoying
a range of recreational and social activities.
Consequently, participant narratives challenge the primary
tenet of the medical model of alcoholism: that it is an incurable
disease. Disease concept proponents would argue that these four
persons have demonstrated merely that they are not alcoholics.
Although this is a possibility, this argument does not acknowledge
the serious nature of each participant’s past troubled relationship
with alcohol. Nor does this argument address the fact that professionals,
and / or fellowship members themselves supported these participants’
inclusion into 12-step culture at one point, thereby accepting
them as "recovering alcoholics." In fact, this argument tends
to reflect the political nature of the disease concept, emphasizing
that disease-focused theory has been constructed in a manner that
prioritizes safest outcomes and risk reduction over self-determination,
strengths, and capacities.
Applications of disease-focused theory (AA, 1976; American
Society of Addiction Medicine, 2000; Canadian Association of Addiction
Medicine, 2002; Diamond, 2000; Gorski & Miller, 1986; Jellinek,
1960) can have a totalizing feel (Le, Ingvarson, & Page, 1995).
Alcohol misuse is often seen as symptomatic of the progressive
illness of alcoholism, requiring abstinence and AA. Mandating
a rigid prescription for least-risky behaviour does not necessarily
honour individual capacities, as attested by the participants
in this research. In respect to the disease model, these participants
demonstrate that not all persons with serious drinking problems
are alcoholics, and that 12-step programs may not suit the needs
and preferences of all persons with a history of serious drinking
problems.
Participants in this study seem to be more effectively supported
using harm reduction perspectives, which also promote safety,
but in the context of individual needs and preferences. While
harm reduction rhetoric does not generally recommend experimenting
with high-risk substances, this perspective accepts the fact that
risky behaviour does occur. Harm reduction principles support
ideas such as using personal guidelines and limits to manage alcohol
use, as well as establishing criteria to assess and, if necessary,
abandon the experiment with controlled.
Practice Implications of this Study
This research presents several implications for social work
practitioners in the addiction field. Participant narratives illustrated
a dilemma regarding assessment: most of the "new relationship
with alcohol" participants were referred to 12-step fellowships
by professionals. How do we effectively distinguish alcoholics,
for whom 12-step referrals are appropriate, from other problem
drinkers? Perhaps there are more effective methods of assessing
client needs and preferences.
Participant narratives also illustrated a potential dilemma
regarding resources. Claire provided an example of an alternative
support community through her participation in a 16 step empowerment
program (Kasl, 1992). In small, northern, and remote communities,
professionals may refer clients to 12-step or other resources
out of immediate necessity, lacking other resources that might
provide a more fitting or effective service. In other words, ethical
practice would indicate referral to the only resources available,
a better-than-nothing scenario. Although all of the participants
who attended a 12-step program in this research indicated gratitude
for the program’s support in gaining a period free from
abusive drinking, there was also significant interest in the development
of accessible alternative resources and support systems.
Advice offered to social workers by participants suggests
a preference for client-centred practice. Client-centred approaches
are supported by the codes of ethics for social workers and addiction
counsellors (British Columbia Association of Social Workers, 1999;
Canadian Association of Social Workers, 1994)
Major Contributions of this Study
This study has provided evidence of possibility. Participants
with serious alcohol problems in their past quit drinking without
using deficit rhetoric associated with the disease model, or they
abandoned the rhetoric and have successfully managed their drinking.
These experiences have happened; this proves that they are a real
possibility. Since my decision to end the information-gathering
phase, I have heard from more people about friends or family members
who have experiences similar to those of the participants in this
study.
This study has made several contributions to the field of
addiction research and social work practice. First, it has documented
the experiences of people who have been marginalized by the rhetorical
assumptions of dominant theoretical frameworks. Second, it has
exposed dominant rhetorical deficit-focused perspectives as only
one way of viewing people’s experiences. Participants’
narratives in this study reflect multiple knowledges, journeys,
roads, and uncharted territories. Third, this research provides
a social constructionist model depicting the negotiation of meaning
between cultures of knowledge, which contribute to the transformation
of identity. This model may have some utility for understanding
experiences of people who choose to live in theoretically uncharted
territories. Finally, this study has drawn several implications
for social work practice, regarding assessment procedures, therapeutic
approach, and resource development.
Conclusion
This study has described the experiences, needs, and preferences
of people who have chosen to address alcohol problems beyond the
rhetoric of the disease model and 12-step framework. In the process,
some of these people have faced marginalization as a consequence
of blazing their own trails through theoretically uncharted territories.
Their narratives helped to explore issues surrounding deficit-focused
paradigms of addiction treatment. They participated in the development
of a social constructionist model to help understand discourse
relating to their experiences. Their narratives demonstrated how
overcoming serious alcohol problems can involve multiple knowledges,
journeys, roads, and uncharted territories in the quest for a
more fulfilling, more meaningful life. Several implications for
social work practice were discussed regarding assessment, therapeutic
approach, and resource development.
One of the most significant concepts of the discipline known
as cultural studies is the idea that knowledge is relative; there
can be no end point. Consequently, there is no conclusion for
this research into alternative experiences and journeys relating
to alcohol problems. I hope that this information will serve to
invite the possibility of openness regarding how we in the helping
profession see and serve the people we are asked to assist.
In summary, the experiences of the participants in this study
contradict rhetorical assumptions that are often the foundation
for strategic practice in the addiction field. Perhaps the best
way to address this point is through the commonly used pickle
metaphor. Essentially, cucumbers can become pickles, but never
vice versa. Yet this research provides evidence of pickles "reclaiming
cucumberhood." This research also clearly documents participants
who were able to stop the pickling process on their own without
professional or conventional help. Finally, this research supports
the social constructionist view of pickles and cucumbers as linguistic
conveniences that serve the viewer more than the person under
gaze.
The persons in this study said they were willing to volunteer
their experiences, providing that their stories might offer hope
and assistance for one other person out there. I respect and reflect
on their sentiment as a personal challenge, and respectfully invite
you, the reader, to consider their ideas when reflecting on your
own practice.
References
AA. (1976). Alcoholics Anonymous (Vol. 3). New York: Alcoholics
Anonymous World Services.
Alasuutari, P. (1992). Desire and craving: A cultural theory
of alcoholism. Albany, NY: State University of New York Press.
Alasuutari, P. (1996). Theorizing in qualitative research: A
cultural studies perspective. Qualitative Inquiry, 2(4),
371385.
American Psychiatric Association. (2000). Diagnostic and statistical
manual of mental disorders (4th ed.). Washington,
DC: Author.
American Society of Addiction Medicine. (2001, August 18). The
definition of alcoholism. Retrieved November 30, 2002, from
http://www.asam.org/Frames.htm.
Anderson, S. C. (1994). A critical analysis of the concept of
codependency. Social Work, 39(6), 677685.
Baker, T. B. (1988). Models of addiction: Introduction to the
special issue [entire issue]. Journal of Abnormal Psychology,
97(2), 115117.
Bannerman, B. B. (2000). A search for healing: A phenomenological
study. Unpublished masters thesis, University of Northern
British Columbia, Prince George, BC.
Berg, I. K., & Reuss, N. H. (1998). Solution step by step:
A substance abuse treatment manual (1st ed.). New
York: W. W. Norton.
Blum, T. C., & Roman, P. M. (1987). Social constructions
and ideologies of substance abuse [entire issue]. Journal of
Drug Issues, 17(4).
British Columbia Association of Social Workers. (1999). Code
of ethics. Vancouver, BC: Author.
Brooker, P. (1999). A concise glossary of cultural theory.
New York: Oxford University Press.
Canadian Association of Social Workers. (1994). Social work
code of ethics. Ottawa, ON: Author.
Canadian Society of Addiction Medicine. (2002, November 27).
Definitions in addiction medicine. Retrieved November 30,
2002, from www.csam.org/index.html.
Chang, J., & Phillips, M. (1993). Michael White and Steve
de Shazer: New directions in family therapy. In S. Gilligan &
R. Price (Eds.), Therapeutic conversations (pp. 95111).
New York: W. W. Norton.
Denzin, N. K. (1993). The alcoholic society: Addiction and
recovery of the self. New Brunswick, NJ: Transaction Publishers.
Diamond, J. (2000). Narrative means to sober ends: Treating
addiction and its aftermath. New York: Guilford Press.
Figgis, M. (1995). Leaving Las Vegas [Motion picture].
United States: Metro Golden Mayer Studios.
Fillingham, L. A. (1993). Foucault for beginners. New
York: Writers and Readers Publishing.
Furman, B., & Ahola, T. (1992). Pickpockets on a nudist
camp: The systemic revolution in psychotherapy. Adelaide,
Australia: Dulwich Centre Publications.
Gorski, T., & Miller, M. (1986). Staying sober: A guide
for relapse prevention. Independence, MO: Herald House/Independence
Press.
Granfield, R., & Cloud, W. (1996). The elephant that
no one sees: Natural recovery among middle-class addicts. Journal
of Drug Issues, 26(1), 4562.
Gubrium, J. F., & Holstein, J. A. (1999). At the border of
narrative and ethnography. Journal of Contemporary Ethnography,
28(5), 561573.
Gusfield, J. R. (1996). Contested meanings: The construction
of alcohol problems. Madison, WI: University of Wisconsin
Press.
Holst, J. A., (2003a, January 18). Advertising mascots: The
Swedish Bikini Team. Retrieved January 18, 2003, from http://www.tvacres.com/admascots_swedishbikini.htm.
Holst, J. A., (2003b, January 18). Animal mascots: The Clydesdales.
Retrieved January 18, 2003, from http://www.tvacres.com/horses_advertising.htm.
Howard, R. (1988). Clean & sober [Motion picture].
United States: Warner Brothers.
Jellinek , E. M. (1960). The disease concept of alcoholism.
New Haven, CT: Hillhouse Press.
Kaiser Youth Foundation. (1997). Directory of substance abuse
services in British Columbia. Vancouver, BC: Kaiser Youth
Foundation & Alcohol and Drug Services, Ministry for Children
and Families.
Kasl, C. (1992). Many roads, one journey: Moving beyond the
12 steps. New York: Harper Collins.
Kearney, M. (1998). Truthful self-nurturing: A grounded formal
theory of women’s addiction recovery. Qualitative Health
Research, 8(4), 495513.
Kytasaari, D. (Producer). (2003). TV Tome. Retrieved January
15, 2003, from http://www.tvtome.com.
Le, C., Igvarson, E. P., & Page, R. C. (1995). Alcoholics
Anonymous and the counselling profession: Philosophies in conflict.
Journal of Counselling and Development, 73, 603609.
Lender, M. E. (1979). Jellinek ’s typology of alcoholism:
Some historical antecedents. Journal of Studies on Alcohol,
40(5), 361375.
Marlatt, G. A. (Ed.). (1998). Harm reduction: Pragmatic strategies
for managing high-risk behaviours. New York: Guilford Press.
Miller, W. R., & Rollnick, S. (1991). Motivational interviewing:
Preparing people to change addictive behaviour. New York:
Guilford, Press.
OHanlon, W. H. (1993). Possibility therapy: From iatrogenic
injury to iatrogenic healing. In S. Gilligan & R. Price (Eds.),
Therapeutic conversations (pp. 321). New York: W. W. Norton.
Peele, S. (1989). Diseasing of America: Addictions treatment
out of control. Lexington, MA: Lexington Books.
Peele, S., & Brodsky, A. (1991). The truth about addiction
and recovery. New York: Fireside.
Prochaska, J. O., Norcross, J. C., & DiClemente, C. C. (1994).
Changing for good: A revolutionary six-stage program for overcoming
bad habits and moving your life positively forward. New York:
Avon Books.
Rabinow, P. (1984). The Foucault reader. New York: Pantheon
Books.
Roberts, G., Ogborne, A., Leigh, G., & Adam, L. (1999a).
Best practices: Substance abuse treatment and rehabilitation.
Ottawa, ON: Office of Alcohol, Drugs and Dependency Issues, Health
Canada.
Roberts, G., Ogborne, A., Leigh, G., & Adam, L. (1999b).
Profile: Substance abuse treatment and rehabilitation in Canada.
Ottawa, ON: Office of Alcohol, Drugs and Dependency Issues, Health
Canada.
Smith, L., & Winslade, J. (1997). Consultations with young
men migrating from alcohol’s regime. In M. Raven (Ed.),
New perspectives on addiction (Vols. 2 & 3, pp. 16–34).
Adelaide, Australia: Dulwich Newsletter.
Sommer, S. (1997). The experience of long-term recovering alcoholics
in Alcoholics Anonymous: Perspectives on therapy. Alcoholism
Treatment Quarterly, 15(1), 7580.
Thomas, B., Topping, J., & Grant, S. (2000), 28 days
[Motion picture] United States: Columbia Tristar.
Truan, F. (1993). Addiction as a social construction: A postempirical
view. Journal of Psychology Interdisciplinary & Applied,
127(5), 489500.
White, M. (1993). Deconstruction and therapy. In S. Gilligan
& R. Price (Eds.), Therapeutic conversations (pp. 2261).
New York: W. W. Norton. |
